I awoke on the floor in the aisle of my United Airlines flight to Los Angeles, with three unfamiliar men crouched around me, bearing serious expressions as they looked down on my prone body.
I was next to my seat. My daughter was crying inconsolably in her seat next to mine, and my wife was calling to me with an urgent tone from the next seat over.
Gradually, as my confusion faded and the men let go of me (I’d been cursing them out, in mangled words because I had bitten my tongue), I became aware that I was in intense pain, I could not move much, and my wife’s words became clearer:
I’d had a seizure. And so our relaxing family holiday, which had only just begun, ended. And so my waking nightmare began.
Stomach-Churning Rating: 5/10; lots of Anatomy Fail CT/x-ray images and gruesome descriptions, and a photo of some bruising.
I was helped back into my seat as I regained my senses, I noticed blood on me from my tongue, and I learned that we were 2 hours away from L.A. As I was acting more normal, and we were 5/6 of our journey along, there was no need to prematurely land the flight. I had fallen asleep while watching “22 Jump Street”, about 1.5 hrs in, and that’s when my seizure struck– much like the previous two seizures I’d had. Jonah Hill could be ruled out as a culprit, but going to sleep was an enabling factor. I got some over-the-counter painkillers and sat in a daze as time ticked by, we landed, and paramedics boarded the plane to whisk me off to the hospital with my family.
Two gruelling days and nights in a California hospital later, with my first night spent in a haze of clinical tests, begging for painkillers, yelling in pain every time I moved, and otherwise keeping my hospital roommate awake, the story became clearer: my seizure was so intense that I’d dislocated my right shoulder (unfortunately I’d not had much pain relief when the emergency room staff popped it back into my glenoid), probably dislocated my left shoulder too but then relocated it myself admist my thrashing, and done this (cue Anatomy Fail images):
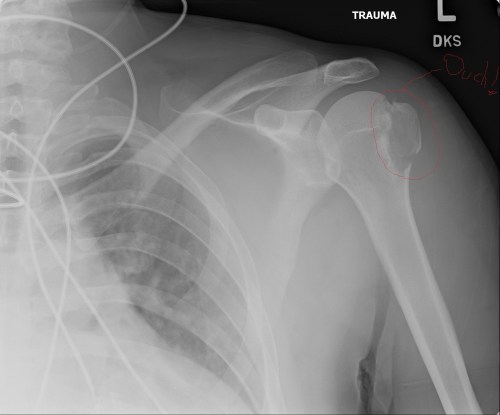
Left shoulder, with the offending greater tubercle/tuberosity of the humerus showing fracture(s).
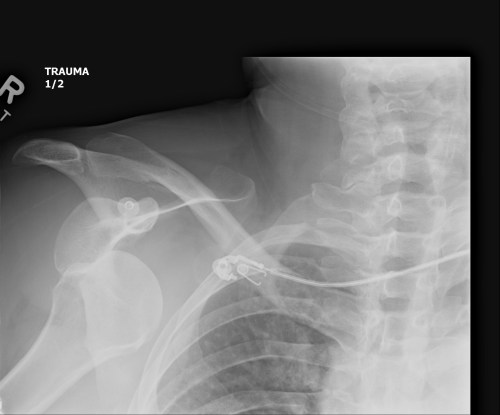
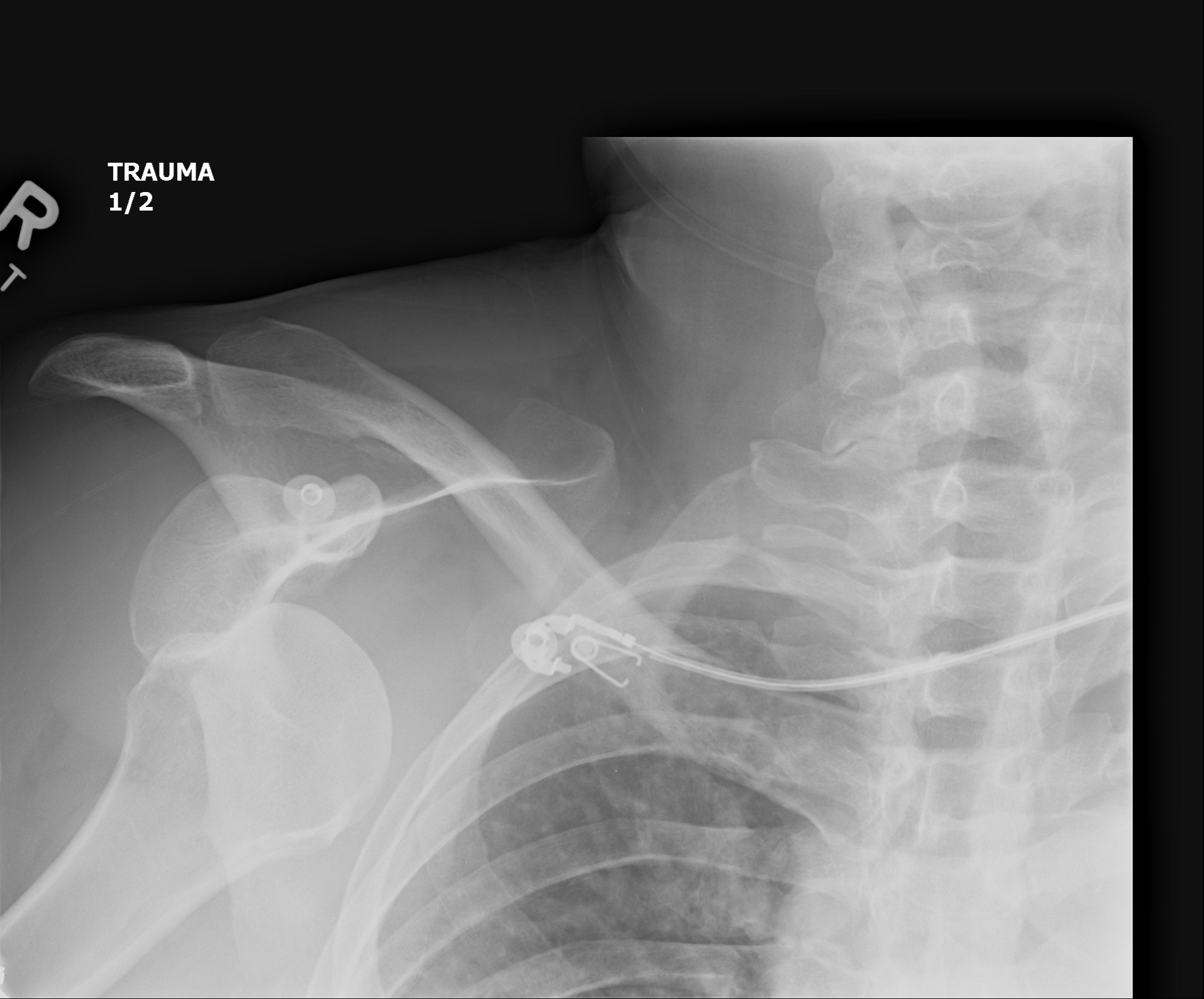
Right shoulder x-ray, showing dislocation of the head of the humerus from the glenoid. Compare with above image- humerus has been shifted down, the shoulder joint is facing you. BUT no fractures, yay!

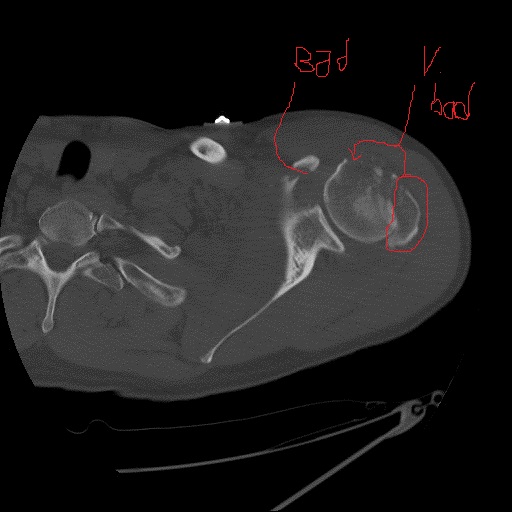
CT scan axial slice showing my spine (on left), then scapula with fractured coracoid process (“Bad”) and displaced, fractured greater tubercle of humerus on right side (“V bad”).
So, that explains most of the pain I was in.
What’s amazing is that the fractures most likely occurred purely via my own uncontrolled muscle contractions. All the karate and weight-training I’d been doing certainly had made me stronger in my rotator cuff muscles, which attach to the greater tubercle of the humerus. And with inhibition of my motoneurons turned off during my seizure, and both agonist and antagonist muscles near-maximally turned on, rapid motions of my shoulders by my spasming muscles would have dislocated my shoulders and then wrenched apart some of the bony attachments of those same muscles. I’m glad I don’t remember this happening.
I had also complained of pain in my neck, so they did a CT scan and x-ray there too:
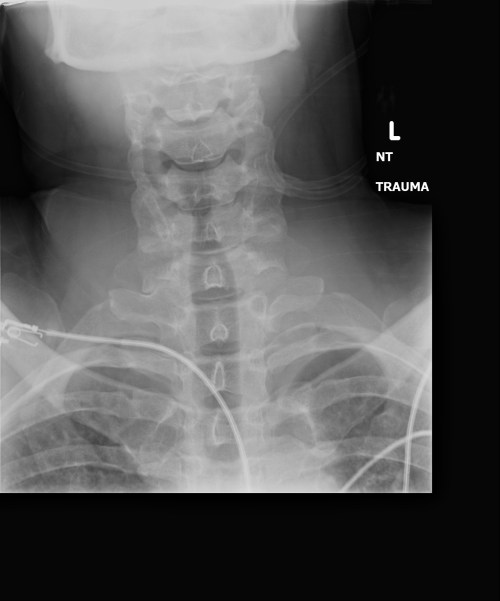
X-ray: No broken neck. This is good. Just muscle strain, which soon faded.
The left shoulder injuries created a hematoma, or mass of blood beneath my skin, and soon that surfaced and began draining down my arm (via the lymphatic system under gravity’s pull), creating fascinating patterns:

Bruises migrating; no pain associated with these, just superficial drainage of old blood. This is tame, tame, tame compared to what my left ribcage looked like. I’ve spared you that.
But then more fundamentally there was the question of, why a seizure? With no clear warning? As I’ve explained before, I’d had a stroke ~12 yrs ago that caused a similar seizure but with no injuries to my postcranial body. So a series of MRI and CT scans ensued (the radiation I’ve had from the latter is good fodder for a superhero/villain origin tale? Marvel, I’ll await your call), and there was no clear damage or bleeding, and hence no stroke evident. Good news.
There are, however, at least two sizeable calcifications in my brain that are likely to be hardened scar tissue from my stroke. These may or may not have an identifiable affect on me or linkage with the seizure. Brain calcifications can happen for a variety of reasons, sometimes without clear ill effects.
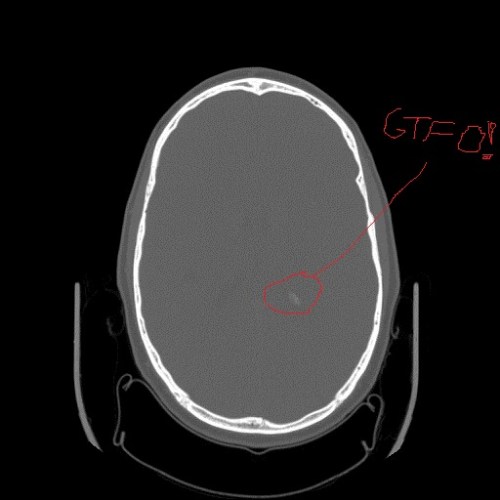
Calcification in parietal lobe of my cerebrum, from axial CT scan slice. But no bleeding (zone of altered density/contrast).
That is the state of the evidence. I’ve since had what semblance of a L.A. family holiday I could manage, benefitting from a touching surge of support from my family, friends and colleagues that has kept me from sinking entirely into despair and has brought quite a few smiles.
The plane flight home was tense. We were in the same seats again and one of the flight attendants recognized us and came to chat, eager to learn what had happened after we left the plane a week ago. He was very nice and the doctors had given me an “OK to fly” letter. But it was an evening flight. I needed to sleep, yet it was clear to me that sleep was no longer the fortress of regenerative sanctity that I was used to it being. Sleep had taken on a certain menace, because it was a state in which I’d now had three seizures. Warily, I drifted off to sleep after having some hearty chuckles at the ending to “22 Jump Street”. And while it was not very restful slumber, it was the friendly kind of slumber that held no convulsive violence within its embrace. We returned home safely.
In a rush, I cancelled my attendance at the Society of Vertebrate Paleontology conference this week, turning over the symposium I’d convened to honour one of my scientific heroes, biomechanist R. McNeill Alexander (who also could not attend due to ill health), to my co-convenors Eric Snively and Andreas Christian (by accounts I heard, all went well). I missed out on a lot of fun and the joy of watching 2 of my PhD students present posters on preliminary results of their research. Thanks to social media and email, however, I’ve been able to catch a lot of the highlights and excitement from that conference in Berlin.That has helped distract me somewhat from other goings-on.
Meanwhile, I’ve been resting, doing a minimal amount of catching up with work, having a lot of meetings with doctors to arrange treatment, and pondering my situation– a lot.
I know this much: I’ve had two violent seizures in a month (the previous one was milder but still bad, and not a story I need to tell here), and so I’m now an epileptic, technically. When and if I’ll have another seizure is totally uncertain, but to boost the odds in my favour I’m on anti-convulsant drugs for a long time now.
In about half of seizure cases, it’s never clear what caused the seizures. What caused my 2002 stroke is somewhat clear, but the mechanism behind that remains a mystery, and my other health problems likewise have a lot of question marks regarding their genesis and mutually causative relationships, if any. The outcome of this new development in my medical history is likely to be: “maybe your brain calcifications and scar tissue helped stimulate your new seizures, but we can’t be sure. The treatment is the same regardless: stay on anti-convulsants for a while, try going off them later, and see if seizures manifest themselves again or not.” Brains are freaking complicated; when they go haywire it can be perplexing why.
As a scientist, I thrill at finding uncertainty in my research topics because that always means there is work left to be done. But in my own life outside of science, stubborn, independent, strong-willed control freak that I can certainly be at times, I am not such a fan of uncertainty. In both cases the goal is to minimize that uncertainty by gathering more information, but in our lives we often encounter unscalable walls of uncertainty that persist because of lack of knowledge regarding a problem that vexes us, especially a medical problem. We then can feel in a helpless state, adrift on the horizon of science, waiting for explorers to push that horizon further and with it advance our treatment or at least our insight into ourselves.
When the subject of that uncertainty is not some detached, objective, unthreatening, exciting research topic but rather ourselves and our own future constitution and mortality, it thus becomes deeply personal and disconcerting. I’m grateful that I don’t have brain cancer or some other clear and present threat to my immediate vitality. Things could be a lot worse; I am here writing this blog after all. I’ll never forget now being in the ambulance and thinking “this may be the end of it all; I might not last much longer”, and choking out a farewell to my wife just in case things took a bad turn. I’m grateful for the amazing things that modern medicine and imaging techniques can do– these have saved my life so many times over, I cannot fathom how to quantify it. And I’m grateful for the people that have helped me through this so far. Fiercely independent as I may be, I can’t face everything alone.
I am reminded of words I read recently by Baruch Spinoza, “The highest activity a human being can attain is learning for understanding, because to understand is to be free.” To further paraphrase him, we love truth because it is knowledge that enables us to stay alive- without it, we are flying blind and soon will crash. With the freedom it brings, we know the landscape of our own life and where the frontiers of uncertainty lie (“here be dragons”).
The past two weeks have been horrendous for me. I’d been feeling healthy and stronger than ever in many ways, and my life as of my birthday a month ago felt pretty damn good. But now everything has come crashing down in disaster, and I have been suffering from the realization, once again, of how vulnerable I am and how little I can control, and the darkness that ushers in as the odds begin to stack up against our future lives. I am acutely aware now of where the “dragons” are.
I am taking one important step forward, though, in wresting life back onto the rails again- this week I undergo surgery to put my left shoulder back together. While that’s scary, to be sliced open and have my rotator cuff and bones carpentered back where they should be, I know I’m in good hands with a top UK shoulder surgeon and methods that are tried-and-true. The risks are small, although the recovery time will be long. There won’t be any hefting of big frozen elephant feet in my research soon, not for me, and so my enjoyable anatomy studies are going to have to change their track for coming months while I regain my strength and rely on others’ help.

(do you know the movie reference? I have a new empathy for Ash.)
Then we’re on to the frightening task of tackling the spasmodic-gorilla-in-the-room with neurologists. We’ll see where that journey leads.
One thing is certain: I’m still me and there’s still a lot of fight left in me, because I have a lot left to fight for, and people and knowledge to aid me in that fight. I can shoulder the burden of uncertainty in my life because I have all that. Off I go…
20 November UPDATE:
I’ve had surgery to put my greater tuberosity back where it belongs. Thanks to a skilled surgeon’s team, some sutures and nickel-titanium staples, I am back closer to my normal morphology and can begin recovering my (currently negligible) shoulder joint’s range of motion via some physiotherapy. Surgery went very well; I was just in hospital for ~30 hours; but the 9 days of recovery since have been brutally hard due to problems switching medications around. Today I got my stitches out and a beautiful x-ray showing plentiful healing; yay!

This is a slightly oblique anterior (front) view of my left shoulder/chest. Fracture callus means healing is working well!
Four surgical staples (bright white thingies on upper RH side of image): forever now a part of my anatomy.
Read Full Post »